
Adrienne Bush isn’t a fan of Medicaid work requirements — or as she, the executive director of the Homeless and Housing Coalition of Kentucky, puts it, “coercing people into minimum wage jobs.” In 32 days, Kentucky will begin rolling out its new Medicaid program that conditions insurance on work, along with a host of other new eligibility requirements. So, now, Bush’s priority is harm reduction.
“Right now I’m very worried about implementation and people falling through the cracks,” Bush told ThinkProgress. “Every forum that either I or one of my colleagues go to, it feels like we get different information.”
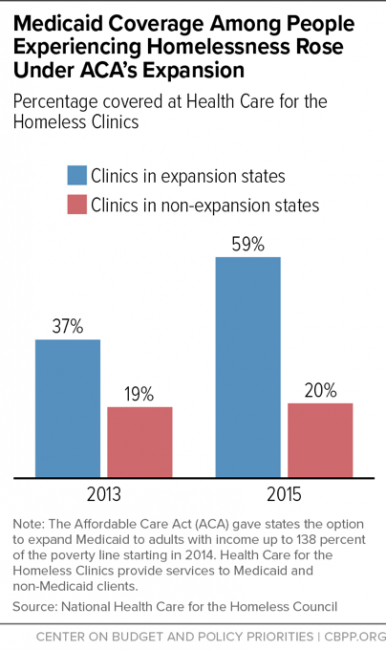
As a result, Bush has had trouble balancing her main job of getting people stable housing, with her new obligation of ensuring those experiencing homelessness stay insured. While those who are homeless can be exempted from the new work requirements under the law’s “medically frail” distinction, they are still required to opt out, in what advocates describe as a confusing process that risks kicking them off the health program. The homeless community is especially vulnerable without insurance, as they experience a mortality rate three to four times higher than the general population.
“The state will say [the different information is] ‘because we’re changing our process based on stakeholder input,'” Bush said. “It’s very frustrating to not know what to expect.”
Bush is one of many consumer advocates trying to protect the state’s recent gains.
Roughly 500,000 people gained health insurance since Kentucky expanded Medicaid eligibility to 138 percent of poverty (or $28,180 for a family of three) in 2014. The state was the Obamacare success story in the South, as Kentucky was an early adopter of health law. It was even heralded for building the best Obamacare website, while Healthcare.gov fumbled.
Then came Gov. Matt Bevin (R). In 2015, he campaigned on ending Medicaid expansion, but when he was elected to office, he took another approach. In August 2016, Bevin asked the federal government to redesign Medicaid expansion, adding a conservative twist in how it is delivered. The Trump administration okay-ed the waiver in January. Now, the state is poised to move 100,000 off Medicaid coverage.
The state claims that those individuals will transition into private insurance, but many, like Bush, are skeptical. They fear that people will accidentally drop coverage as they try to navigate a complicated Medicaid program in which people living near the poverty level have to pay premiums and report 80 hours of work per month. If they miss two payments, don’t report enough hours or report it incorrectly, or just forget to submit insurance renewal paperwork on time, they will lose coverage for six months.
“We’ll see what happens now as states are asking for waivers to increase what are effectively paperwork burdens.”
It’s not just Kentucky. The Trump administration has permitted three other states to take similar measures. While Medicaid expansion is arguably the most successful provision under Obamacare, its fate is now uncertain.
“We’ll see what happens now as states are asking for waivers to increase what are effectively paperwork burdens,” health law professor at Washington and Lee University Tim Jost told Kaiser Health News.
Health care is already complicated, and Kentucky’s new Medicaid program gets even more complicated, requiring enrollees to manage two to three health accounts. The burden will rest largely on vulnerable groups. While the state will exempt many groups — like those experiencing chronic homelessness, substance use disorder, or domestic violence — from forthcoming changes, consumer advocates are still concerned individuals will trip up when applying for immunity, especially considering even state officials can trip up when explaining the details.
A confusing process
“The biggest cause for concern is just all of the tripwires involved with this waiver,” said Dustin Pugel of the Kentucky Center for Economic Policy, referring to all the ways people could accidentally lose coverage, and not because they’re not meeting their work, volunteer, or job training requirements.

Indeed, the new Medicaid program goes beyond work requirements. But is the state telling people about all the changes and if those changes even apply to them? It’s complicated, said Pugel.
Pugel has attended numerous forums where state officials have informed the public about the waiver, dubbed Kentucky HEALTH. At the last one he attended in early May, he recounted an instance in which two officials contradicted themselves. When asked if people who are automatically exempted from paying premiums would be sent a warning letter, the official leading the discussion said “no,” while another said “yes,” with the caveat that not everyone will have to pay.
At the third “Stakeholder Advisory Forum” for the changes to #Kentucky’s Medicaid program, estimated to knock off 100,000 people from coverage. #InsureKY pic.twitter.com/kWfrsyNLVH
— Dustin Pugel (@Dpugel) May 3, 2018
“Even in public presentations they’re uncovering things that should not be the way they are,” Pugel told ThinkProgress. “They keep changing different aspects of the waiver as we go forward because they had not — I don’t think — done sufficient planning before it was approved to be able to make sure that everybody who needs coverage is going to get coverage in some way.”
“The biggest concern is how all these changes are going to be communicated with Medicaid members,” said Jason Dunn of Kentucky Voices for Health. Recipients will likely turn to advocates or providers for answers, but they don’t always have them.
This is largely due to the fact that the state doesn’t always communicate changes to key stakeholders. In early May, for instance, the state said people who experience homelessness for 12 consecutive months or for four different occasions totaling 12 months over three years could apply for a “medically frail” exemption. But last week, after advocates like Bush and Dunn called for expanding the definition, Kentucky officials backtracked and said anyone who experiences homelessness for three months will be exempt. Bush only learned about the recent changes after ThinkProgress reached out to her in a follow-up email.
While the state employs “assisters,” who are paid to help members navigate Medicaid, it hasn’t hired any new enrollment assisters for the roll out.
State officials did not return ThinkProgress’ multiple requests for comment.
Vulnerable groups, like the homeless, are in jeopardy
“There are probably going to be a lot of people who try to do everything they can the right way, but still end up losing coverage just because the system is going to be so complex and tricky and hard to navigate,” Dunn told ThinkProgress.
Take the “medically frail” exemption, for instance. To get a temporary six-month exemption from the work requirements, people filling out the online application must answer “yes” to the question “are you in poor health?” The “yes” will then prompt a second question, where they’ll be asked if they are chronically homeless. People could misinterpret the first question and then miss the opportunity to self attest to experiencing homelessness, said Dunn.
To get a full-year exemption, individuals must complete the form with a medical provider.
“To me, this flies in the face of trauma informed care,” said Bush, who has worked on homelessness issues for 10 years. “It’s asking people to tell their story over and over and over again and report on this and report on that.”
Not only can the added paperwork be confusing, but there is also no guarantee that people will commit to filling out the necessary forms or just forgo coverage after six months.
“Because if you are living in a parking garage … you’re not going to be able to follow up,” said Bush. “Maybe you will be, maybe, I don’t know. I’m just thinking about if I were experiencing homelessness what would I prioritize? I would prioritize finding a place to sleep at night.”

The hope is to identify people experiencing homelessness in other ways. One idea was to automatically exempt the number of people — of the 4,025 experiencing homelessness — that are on Medicaid. The Kentucky Housing Authority’s Jeremy Ratliff, who tracks this population, told ThinkProgress “we have been working with [the Department for Medicaid Services]” ahead of the roll out so they can at least combine data sets, but “[u]nfortunately, it is still very much a work in progress.”
Kentucky’s Medicaid waiver process has, so far, been very different from the ACA roll out.
Frankfort came to us during the ACA roll out, Bush said. At the time, an enrollment assister called a “Kynector” (named after the state’s former health exchange, Kynect, which Bevin ended in 2016) stopped by at the homeless shelter where she worked. But now, Bush has to go to Frankfort, meaning she needs to ask for a meeting or attend a public forum in person in order to obtain necessary information and resources. (The forum in May was in Frankfort, but not all forums take place in the state capital.)
It didn’t have to be this way, advocates argued. Nearly 40 organizations, from the American Heart Association and AARP Kentucky, asked that the state create a formal stakeholders advisory council, like the one created for Obamacare, to help shepherd changes. But officials declined, claiming their forums were sufficient.
“If they’re genuinely trying to improve people’s health and make sure that there are systems that empower people to become healthier then I guess my question is why have you created a system that is so complicated?” said Pugel.
“[State officials are] often confused by what they’re creating, and yet they’re turning around and expecting low wage workers, people with disabilities, and some of our most vulnerable — who are doing enough just to try and get by — to manage a health insurance program that is far more complicated than any I’ve experienced… I am deeply concerned by the level of confusion that this is creating and I am not confident that the state is up to the task of clearing up that confusion by July 1st.”